Short Communication
The Link between Increased Body Mass Index and Radiotherapy of Childhood Leukemia: The Need to Manage Obesity in Pediatric Leukemia Patients
Minyoung Lee and Eun Ju Kim*
Division of Basic Radiation Bioscience, Korea Institute of Radiological and Medical Sciences, Korea
*Corresponding author: Eun Ju Kim, Division of Basic Radiation Bioscience, Korea Institute of Radiological and Medical Sciences, Korea
Published: 22 Mar, 2017
Cite this article as: Lee M, Kim EJ. The Link between
Increased Body Mass Index and
Radiotherapy of Childhood Leukemia:
The Need to Manage Obesity in
Pediatric Leukemia Patients. Clin
Oncol. 2017; 2: 1240.
Keywords
Radiotherapy; Body mass index; Obesity; Childhood leukemia; Acute lymphoblastic leukemia
Short Communication
Although radiotherapy is one of the most important modalities used to cure cancer, radiation
exposure can damage the human body. There is great debate regarding the health risks of radiation
on metabolism, but strong epidemiological evidence argues that radiotherapy of childhood leukemia
may be linked with an increase of body mass index. This short report seeks to summarize these
epidemiological data and the apparent alteration of certain obesity-related genes in radiotherapytreated
childhood leukemia patients. Although radiation is considered to be unfavorable for the
preservation of metabolic homeostasis, we further propose that pediatric leukemia patients need
interventions to control metabolic dysfunction and prevent subsequent obesity.
Radiotherapy increases the body mass index of patients with childhood leukemia
The use of radiation has increased tremendously in modern years, and many humans
have been exposed to medical radiation. Radiotherapy (RT) has become an essential part of the
treatment of childhood cancer; it improves survival for some of the most common malignancies,
including lymphoid leukemia, which accounts for 76% of all leukemia cases in children [1,2].
Cranial Radiotherapy (CRT) is part of an effective multimodality therapy that has been used to
treat and prevent the spread of childhood Acute Lymphoblastic Leukemia (ALL) [3]. Allogeneic
stem-cell transplantation, which is the treatment of choice for some leukemia patients, requires
Total Body Irradiation (TBI) as a conditioning therapy that suppresses the recipient’s immunity
to allow sustained engraftment, prevent rejection, and eradicate tumor cells [4]. Abdominal
radiation is another important tool used in the treatment of many childhood cancers, including
neuroblastoma, soft tissue sarcomas, and Wilms tumor [5]. Unfortunately, however, almost 75% of
survivors of childhood ALL have chronic health conditions that negatively impact their morbidity
and mortality [6]. RT has been associated with increased risks for late mortality, the development
of cancer, the acquisition of pulmonary, cardiac, and thyroid dysfunctions, and an increased overall
risk for chronic health conditions [3]. Overweight and obesity are frequently seen following RT
for childhood ALL, andstrong epidemiological evidence links RT of childhood ALL with increased
body mass index (BMI) [6-12] (Table 1). BMI is a statistical measure of human weight scaled
according to height; both BMI and its alteration appear to be comprehensive indicators of health
status. However, although it is generally accepted that obesity is one of the most common late effects
seen among childhood ALL survivors, the radiobiological mechanisms of radiation-induced obesity
in RT-treated childhood leukemia patients are not well understood.
Genetic contributors to obesity in survivors of RT-treated childhood leukemia
Generally, Ionizing Radiation (IR) stimulates both pro-and anti-proliferative signaling pathways
to create an imbalance in cell fate decision. IR can regulate numerous genes and factors involved
in DNA damage and repair, cell-cycle progression, cell death, and various intracellular radiationdependent
responses [13]. IR induces the abundant production of Reactive Oxygen Species (ROS),
and increased cellular levels of ROS cause oxidative damage to DNA, providing a mechanistic basis
for the ability of radiation to cause DNA damage and affect cell division [14]. RT-related obesity
appears to be related more to metabolic dysfunction and over-activation of nutrient-sensing
mechanisms than to radiation-induced oxidative stress or DNA-damage responses. However,
some investigations have found that the main energy-sensing signaling pathways could be linked to radiation-induced DNA damage signaling [15]. Therefore, we need to better understand these metabolic alterations and generate additional
data confirming that IR can induce the metabolic abnormalities.
Several genetic association studies have evaluated potential genetic
risk factors for obesity among adult survivors of childhood ALL. Ross
et al. [16] reported that female survivors (N = 600) with BMI ≥25
mg/m2 (i.e., overweight) or obesity were twice as likely as those with
BMI <25 mg/m2 to be homozygous for the Arg allele at residue 223
of the leptin receptor gene (LEPR; Gln223Arg, rs1137101) [16]. This
finding is consistent with other reports suggesting that leptin levels
are increased in female survivors of childhood ALL, and that soluble
leptin receptor levels are negatively correlated with body mass [17].
Leptin, which is among the best known hormones for obesity, exerts
pleiotropic effects on multiple organs and is important for the central
and peripheral signaling that maintains energy homeostasis [18].
Therefore, the absence of leptin activity in childhood ALL patients
with genetic variations of leptin receptor genes may lead to morbid
obesity. Another group of investigators evaluated associations
between obesity and Single Nucleotide Polymorphisms (SNPs) of
the Fat Mass and Obesity-associated (FTO) gene, which was the gene
to be reproducibly associated with human body mass [19]. Among
ALL survivors treated with CRT, they found lower rates of obesity
in those homozygous for the T allele at rs9939609 compared to those
with at least one copy of the A allele [20]. Early study of FTO gene
expression indicated that it was highly expressssed in the brain and
hypothalamus [21]. This is interesting because the hypothalamus is a
major site responsible for controlling the energy balance, and genes
responsible for obesity are known to function in the hypothalamus.
While the exact function of the FTO gene is not yet known, it has
been associated with the regulations of energy homeostasis, body size,
and body fat accumulation. Wilson et al. [22] conducted a genetic
study among 1996 adult survivors of childhood cancer (42% were
ALL survivors) and found potential genetic predictors of obesity on
chromosomes 13 (FAM155A), 2 (SOX11), 4 (GLRA3), and 5 (CDH18
and BASP1) among those exposed to CRT. FAM155A is expressed
in the hypothalamus and pituitary; GLRA3 encodes a receptor
protein involved in glycine neurotransmitter signaling; and CDH18
and SOX11 influence neuronal function. Thus, these findings may
support the hypothesis that CRT-induced brain damage influences
obesity. Although association does not mean causation, these findings suggest that we should undertake large genome-wide linkage
studies and candidate gene connection studies in RT-treated patients
of childhood ALL, in the hopes of helping them cope with overweight
and obesity.
Perspective: Supposing interventions for controlling
obesity in children
Treatment advances have improved the 5-year survival rates
for children diagnosed with lymphoid leukemia to over 90% [1]. To
our knowledge, there have been relatively few reports concerning
overweight both during and after RT of childhood ALL patients. The
early onset of obesity and its persistence into adulthood is arguably
one of the most significant chronic health situations in childhood
leukemia survivors, who are also at increased risk for progressive
cardiovascular and metabolic co-morbidities. Understanding
the etiology of obesity in radiation-exposed childhood leukemia
survivors is an important public health concern given the recent
epidemic rise in obesity rates in the pediatric population worldwide.
To track the extent to which elevated BMI persists after the
completion of RT, it will be essential for future studies to develop
or assess specific blood biomarkers related with increased BMI, such
as leptin, glucose, insulin, cholesterols, etc. In addition to facilitating
the development of new treatments, learning about how these
biomarkers are associated with RT-related weight gain may help
us critically improve the existing clinical interventions. If we hope
to prevent obesity and metabolic syndrome in survivors, we will
need evidence-based intervention strategies that are tailored to the
specific demands of children who are undergoing or have recently
completed RT. Although the existing guidelines on lifestyle changes
aimed at controlling obesity in the general population (e.g., aspects
of diet and exercise) can be valuable for ameliorating obesity and
metabolic syndrome in survivors, further research should evaluate
survivor-specific interventions for monitoring metabolic status and
providing targeted education on nutrition and physical activity. Data
from long-term studies in large survivor cohorts should be used to
inform the most appropriate strategies for medical management
in this distinctive pool of childhood and adolescent patients, and
to develop adjuvant interventions to treat obesity. Patients who
receive RT should be followed up throughout their lives to track
and address the development of RT-associated metabolic syndrome.
Radiobiologists might study the mechanisms of radiation-induced
metabolic dysfunction and search for serum biomarkers that
may be used to estimate the obesity risk of RT-treated childhood
ALL patients. Clinicians should be aware of the late effects in this
susceptible population; they should screen for dyslipidemia and
hypertension and generate risk factor profiles for obesity, diabetes,
and cardiovascular issues, in order to promote better healthcare for
childhood cancer survivors. Finally, governments around the world
should continue to promote health-promotion programs to cope
with obesity issues among pediatric leukemia patients.
Table 1
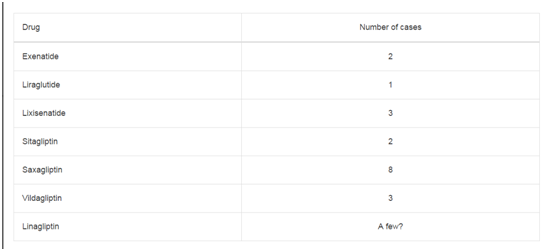
Table 1
Summary of studies on radiotherapy related to increase of BMI in acute
lymphoblastic leukemia patients.
References
- Siegel RL, Miller KD, Jemal A. Cancer Statistics. CA Cancer J Clin. 2017; 67: 7-30.
- Armstrong GT, Stovall M, Robison LL. Long-term effects of radiation exposure among adult survivors of childhood cancer: results from the childhood cancer survivor study. Radiat Res. 2010; 174: 840-850.
- Follin C, Erfurth EM. Long-Term Effect of Cranial Radiotherapy on Pituitary-Hypothalamus Area in Childhood Acute Lymphoblast ic Leukemia Survivors. Curr Treat Options Oncol. 2016; 17: 50.
- Gyurkocza B, Sandmaier BM. Conditioning regimens for hematopoietic cell transplantation: one size does not fit all. Blood. 2014; 124: 344-353.
- Bolling T, Willich N, Ernst I. Late effects of abdominal irradiation in children: a review of the literature. Anticancer Res. 2010; 30: 227-231.
- Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006; 355: 1572-1582.
- Oeffinger KC, Mertens AC, Sklar CA, Yasui Y, Fears T, Stovall M, et al. Childhood Cancer Survivor S: Obesity in adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2003; 21: 1359-1365.
- Garmey EG, Liu Q, Sklar CA, Meacham LR, Mertens AC, Stovall MA, et al. Longitudinal changes in obesity and body mass index among adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2008; 26: 4639-4645.
- Janiszewski PM, Oeffinger KC, Church TS, Dunn AL, Eshelman DA, Victor RG, et al. Abdominal obesity, liver fat, and muscle composition in survivors of childhood acute lymphoblastic leukemia. J Clin Endocrinol Metab. 2007; 92: 3816-3821.
- van Waas M, Neggers SJ, van der Lelij AJ, Pieters R, van den Heuvel-Eibrink MM. The metabolic syndrome in adult survivors of childhood cancer, a review. J Pediatr Hematol Oncol. 2010; 32: 171-179.
- Oudin C, Simeoni MC, Sirvent N, Contet A, Begu-Le Coroller A, Bordigoni P, et al. Prevalence and risk factors of the metabolic syndrome in adult survivors of childhood leukemia. Blood. 2011; 117: 4442-4448.
- Jarfelt M, Lannering B, Bosaeus I, Johannsson G, Bjarnason R. Body composition in young adult survivors of childhood acute lymphoblastic leukaemia. Eur J Endocrinol. 2005; 153: 81-89.
- Iliakis G, Wang Y, Guan J, Wang H. DNA damage checkpoint control in cells exposed to ionizing radiation. Oncogene. 2003; 22: 5834-5847.
- Mikkelsen RB, Wardman P. Biological chemistry of reactive oxygen and nitrogen and radiation-induced signal transduction mechanisms. Oncogene. 2003; 22: 5734-5754.
- Sanli T, Steinberg GR, Singh G, Tsakiridis T. AMP-activated protein kinase (AMPK) beyond metabolism: a novel genomic stress sensor participating in the DNA damage response pathway. Cancer Biol Ther. 2014; 15: 156-169.
- Ross JA, Oeffinger KC, Davies SM, Mertens AC, Langer EK, Kiffmeyer WR, et al. Genetic variation in the leptin receptor gene and obesity in survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2004; 22: 3558-3562.
- Tonorezos ES, Vega GL, Sklar CA, Chou JF, Moskowitz CS, Mo Q, et al. Adipokines, body fatness, and insulin resistance among survivors of childhood leukemia. Pediatr Blood Cancer. 2012; 58: 31-36.
- Triantafyllou GA, Paschou SA, Mantzoros CS. Leptin and Hormones: Energy Homeostasis. Endocrinol Metab Clin North Am. 2016; 45: 633-645.
- Speakman JR. FTO effect on energy demand versus food intake. Nature. 2010; 464.
- Szymon S, Bik-Multanowski M, Balwierz W, Pietrzyk JJ, Surmiak M, Strojny W, et al. Homozygosity for the rs9939609T allele of the FTO gene may have protective effect on becoming overweight in survivors of childhood acute lymphoblastic leukaemia. J Genet. 2011; 90: 365-368.
- Gerken T, Girard CA, Tung YC, Webby CJ, Saudek V, Hewitson KS, et al. The obesity-associated FTO gene encodes a 2-oxoglutarate-dependent nucleic acid demethylase. Science. 2007; 318: 1469-1472.
- Wilson CL, Liu W, Yang JJ, Kang G, Ojha RP, Neale GA, et al. Genetic and clinical factors associated with obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer. 2015; 121: 2262-2270.